Multi-Specialty Group: 92 Clinicians, 3.1 Hours Saved Daily

A 92-clinician multi-specialty group used annual engagement-survey data as the wedge for a documentation-focused EHR strategy — and rolled out specialty by specialty, not location by location.
Business Challenges
The annual provider engagement survey at the 92-clinician multi-specialty group landed in the CMO's inbox in February. The headline finding was unambiguous: 38% of clinicians named documentation burden as their #1 reason for considering leaving within 24 months. The number was higher in primary care (49%) and lower in surgical specialties (22%). The CMO took it to the board.
What he proposed was unusual. Most documentation-focused engagements at multi-specialty groups try to standardize across specialties — pick a tool, train everyone, declare victory. The CMO had been at the group for seven years and knew that wouldn't work.
The eight specialties had different note structures, different billing patterns, different malpractice exposures, and different cultural relationships with charting. Internal medicine's documentation problem was not orthopedics' documentation problem. Treating them as the same would produce eight half-solutions.
- Provider engagement survey: 38% groupwide cited documentation as the top reason they might leave; the figure was 49% in primary care and 47% in family medicine.
- Six providers — five primary care, one endocrinology — had given notice over the prior 18 months; exit interviews named documentation in five of six cases.
- Internal benchmarking against MGMA peers showed the group's charting-time-per-encounter was 21% above the median across primary care and 14% above in surgical specialties.
- Specialty-level template inconsistency was driving 22% rework on downstream coding; each specialty's documentation was being re-touched by an external coding vendor.
- Same-day urgent access was capped at 86% of demand — the missing 14% was being routed to urgent care because primary care providers couldn't fit additional encounters into their charting day.
Solution
The CMO ran an internal RFP that was structured around one question: which vendor would commit to deploying specialty by specialty rather than insisting on a single global template? Three vendors made it to the final round. Two declined to commit; their playbook was built around one configuration approach per organization. eCareScribe accepted the constraint and proposed an eight-specialty configuration program.
What unlocked the conversation was that eCareScribe's lead solutions engineer had previously been a practicing internist. He sat with the primary-care lead in a half-day session and rebuilt the primary-care progress note structure from scratch — informed by what primary care actually billed, what was actually defensible, and what an internist actually wanted to look at the next time they saw the patient. That output became the primary-care configuration. The same exercise was run with each of the other seven specialty leads.
The result was eight different progress-note generators behind one platform. Each one looked, to the clinician using it, like a tool built for their specialty. Behind the scenes, eCareScribe's engineering team had abstracted the shared infrastructure (ambient capture, EHR write-back, code suggestion) so that adding the next specialty did not require rebuilding the platform.
Value Delivered
The group tracked four headline numbers across the deployment: provider-reported charting time per encounter, after-hours minutes, encounter throughput, and the next-year provider engagement survey result. The first three moved within the first specialty's pilot quarter; the fourth had to wait for the annual cadence.
- 3.1 hours saved per provider per day on average, with variation by specialty: primary care saved 3.8 hours, family medicine 3.4, orthopedics 2.1, and anesthesiology 1.7.
- 22% encounter throughput lift in primary care; 18% in family medicine; 14% across surgical specialties.
- Documentation as top exit risk dropped from 38% to 11% on the following year's engagement survey.
- Three providers who had given notice retracted their notices; the practice did not lose another provider to documentation in the 18 months following deployment.
- 96.4% first-pass coding accuracy on AI-drafted notes across specialties — within 1.2 points of the senior-coder team's own first-pass rate.
Solution Provided
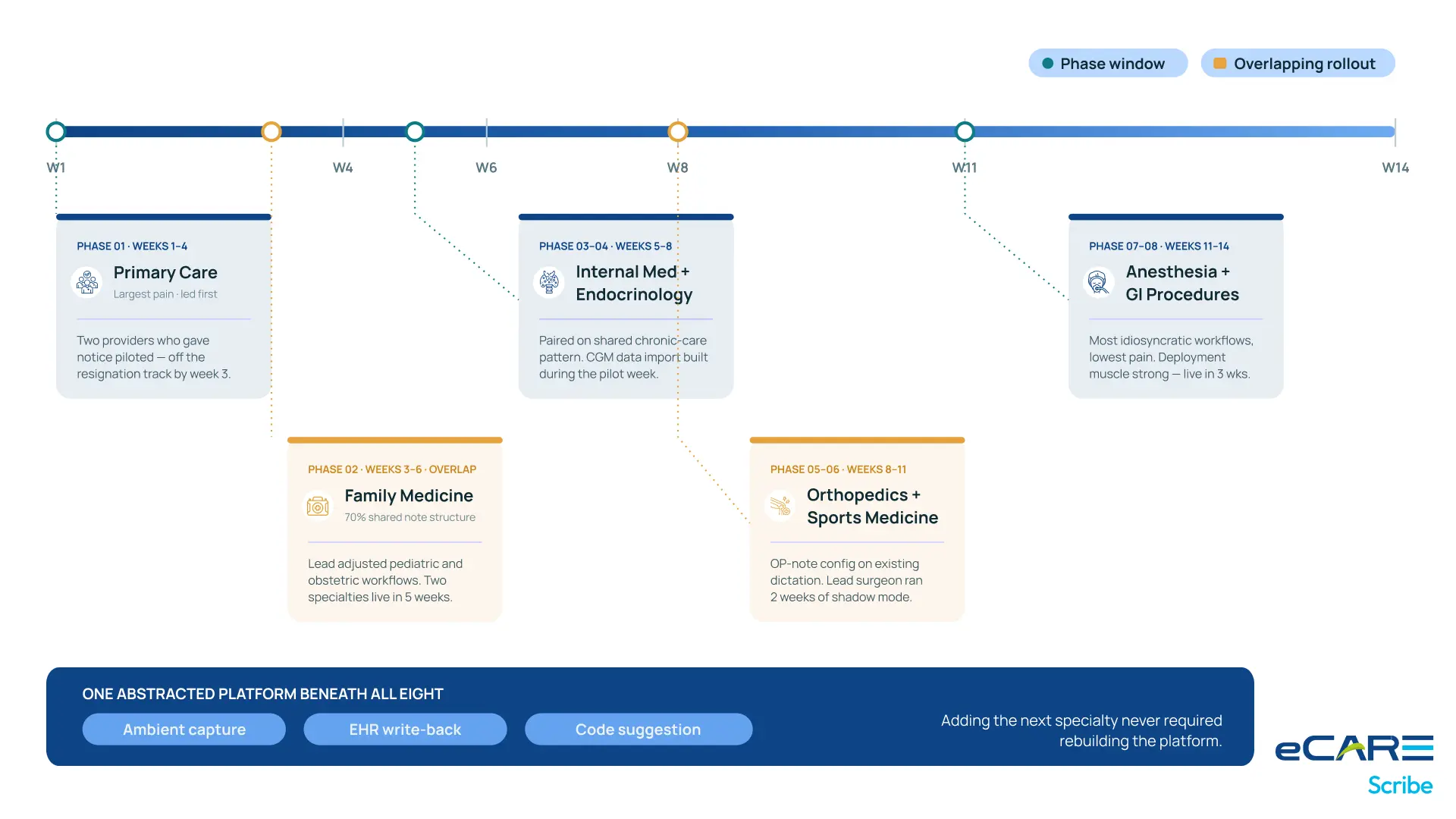
The deployment took 14 weeks, longer than typical, because phasing by specialty rather than location meant eCareScribe was effectively running eight distinct sub-projects in parallel.
Specialty 1: Primary Care (Weeks 1–4)
Primary care went first because the problem was largest there and the political momentum was strongest. The pilot included two of the providers who had given notice. Both were on the system and not in the resignation conversation by week 3.
Specialty 2: Family Medicine (Weeks 3–6, overlapping)
Family medicine started overlapping with primary care because the underlying note structure was 70% the same. The family medicine lead made the structural adjustments needed for their pediatric and obstetric workflows. Two specialties came up in five weeks total.
Specialties 3–4: Internal Medicine + Endocrinology (Weeks 5–8)
The cognitive specialties came up together because they shared a chronic-care documentation pattern. Endocrinology required additional configuration around continuous glucose monitor data import; the eCareScribe team built it during the pilot week.
Specialties 5–6: Orthopedics + Sports Medicine (Weeks 8–11)
Surgical specialties came up next, with an OP-note configuration that piggybacked on existing dictation patterns. Orthopedic surgeons were the most skeptical of any group; the lead surgeon insisted on running the system in shadow mode for two weeks before committing.
Specialties 7–8: Anesthesia + GI Procedures (Weeks 11–14)
Procedural specialties came last because they had the lowest pain and the most idiosyncratic workflows. By the time they came up, the deployment muscle was strong and they were live in three weeks.
The total deployment burned more vendor hours than a standard rollout would. The CMO has been clear that the additional cost was the right investment — what they bought was clinician trust across eight specialties, not just a contract.
Business Value
The CMO's board presentation 18 months after deployment was titled "What we bought." He spent the first slide on the financial numbers and the rest of the deck on the operational ones.
Three categories of permanent gain
First, throughput. The 22% lift in primary-care encounters meant the group could absorb its own urgent-access demand instead of sending it to competitors. That created customer-acquisition velocity the group hadn't seen since pre-pandemic.
Second, recruiting. The provider engagement survey result became a recruiting tool. Job postings now reference the documentation environment as a differentiator. Senior providers from competitor groups have specifically cited the documentation environment in their decision to interview at the group.
Third, financial stability. The reduced exit pipeline took $4.8M of replacement-hiring cost off the operating model. That cost had been silently absorbed into the previous fiscal year's compensation analysis; once it was visible, the board could redirect it.
Why the specialty-by-specialty approach mattered
The CMO has talked publicly about the engagement, and the line he returns to is this: "Multi-specialty groups fail at documentation transformation when they pretend they're a single specialty. We weren't. We never have been. Buying a platform that respected that was the unlock."
What's next
The group is now extending the eCareScribe partnership into its care-coordination program. The same eight-specialty-respect logic is being applied to how chronic-care management documentation is structured. The CMO does not expect that engagement to take 14 weeks. The trust is already built.

