Orthopedic Group: 28% More Surgical Cases per Week

An 18-surgeon orthopedic group needed to add two surgeons in 2026 — and the math wouldn't work until they solved the operative-report backlog. They didn't add the surgeons. They didn't need to.
Business Challenges
The strategic planning meeting in October 2025 had a single agenda item that wouldn't close: should Pinnacle Orthopedic Surgical Group hire two additional surgeons for the 2026 fiscal year? The capacity model said yes — surgical demand at the 4 ASCs was running 18% above what current capacity could absorb. The operating model said no — the practice's existing surgeons were already at the cap of their personal sustainability, and the marginal cost of two additional surgeons (compensation, benefits, ASC time, support staff) wouldn't pencil if existing surgeons remained capacity-constrained.
The bottleneck wasn't OR time. It was an operative report. Pinnacle's surgeons collectively averaged 6 hours of weekly documentation burden — almost all of it dictation catch-up. The dictation transcription queue was running 72 hours behind. Op-notes that had to be finalized within 24 hours for compliance were being signed off late. Complex spinal cases, which had grown to 38% of the case mix, generated 2x the dictation time per case of joint replacements. The math added up to a capacity ceiling that no amount of OR optimization could break.
- Operative-report dictation queue running 72 hours behind, with 14% of op-notes finalized after the 24-hour compliance window.
- Complex spinal case mix had grown from 22% to 38% in two years; per-case dictation time on spinal grew from 11 minutes to 26 minutes.
- Each surgeon was losing approximately 6 OR-time hours per week to documentation catch-up — effectively 0.75 cases per surgeon per week of capacity loss.
- Anesthesia and surgical-assistant documentation lived in separate systems, requiring 11 minutes of manual cross-reconciliation per case from the surgical coordinator.
- The decision to hire two additional surgeons was deadlocked because the COO's model showed it would lock in the existing per-surgeon productivity loss at a larger scale.
Solution
The CFO ran the procurement. Her framing was deliberately financial: "If we can recover one OR case per week per surgeon, we don't need to hire. If we can recover two, we can defer the hire by 18 months and use the savings to recapitalize the ASCs." The discussion of eCareScribe started in that financial frame, not as a clinical productivity tool.
The selection conversation centered on three constraints. First, the platform had to handle surgical dictation patterns, not outpatient progress-note patterns. Most ambient AI products were built for clinic-style encounters; very few handled the dictation cadence and op-note structure of a complex spinal case.
Also, the configuration had to respect the surgeons' existing patterns — Pinnacle's senior surgeons had 15+ years of dictation habit and would not retrain. Third, the platform had to write op-notes that could be cosigned without surgeon editing in more than 90% of cases.
eCareScribe was selected after a single-surgeon proof-of-concept with Dr. Marcus Reedman, the practice's most senior spinal surgeon and the one who had never dictated less than 12 minutes per case in his 22 years. Dr. Reedman ran the system for two weeks. At the end of week two, he called the CFO and said, "I'm getting my evenings back. Sign the contract."
Value Delivered
The CFO tracked one number above all others: cases per surgeon per week. The headline result wasn't the hire-deferral decision (which it eventually became) — it was that the practice's existing 18 surgeons absorbed the demand that the strategic plan had said required two new hires.
- 14 → 18 cases per surgeon per week, a 28% lift achieved without any change to OR scheduling or staffing.
- 72-hour dictation backlog cleared within 6 weeks of full deployment; the practice has not run a backlog since.
- 100% of op-notes finalized within 24 hours; 94% within 2 hours of case completion.
- $3.6M additional surgical revenue in the first 12 months, against an implementation investment of $480K.
- Hiring decision deferred 18 months; the capital that would have funded compensation was redirected into ASC equipment refresh.
Solution Provided
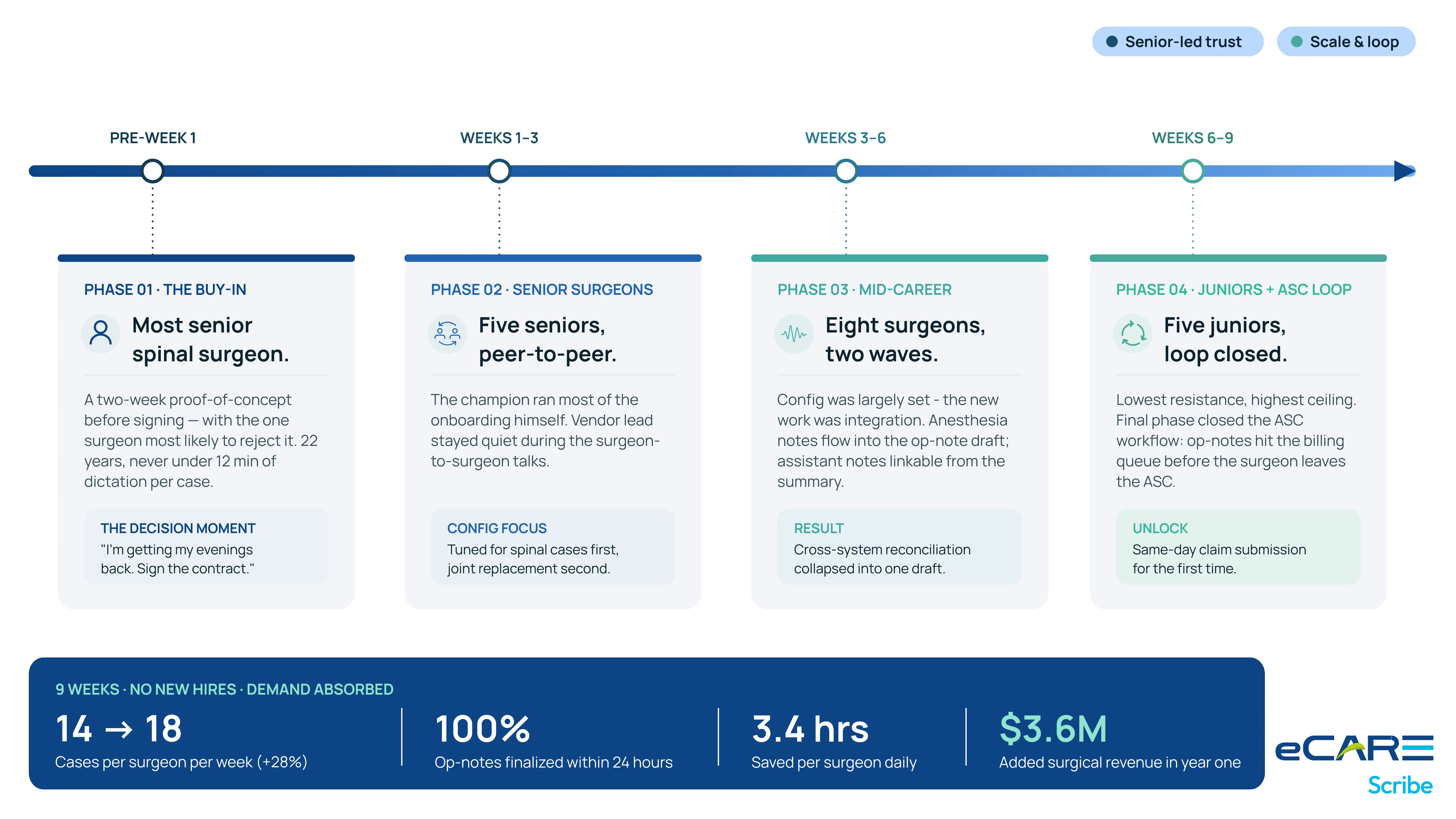
The deployment took 9 weeks total, but felt longer because the cultural work was front-loaded. Surgical groups don't deploy by phases the way primary care does — they deploy by personalities.
Pre-Week 1: The Reedman Buy-In
Before the contract was signed, eCareScribe agreed to a two-week proof-of-concept with Dr. Reedman alone. Reedman was selected because he was both the most respected senior surgeon and the one most likely to reject the system. The unwritten rule of surgical groups is that senior surgeon endorsement is the only currency that moves a deployment. Reedman's call to the CFO at the end of the POC ("Sign the contract") was the actual decision moment.
Weeks 1–3: The Senior Surgeons
The five most senior surgeons came up next. Reedman did most of the peer-to-peer onboarding himself. eCareScribe's deployment lead was present but kept quiet during the surgeon-to-surgeon conversations. The configuration was tuned for spinal cases first, joint replacement second.
Weeks 3–6: The Mid-Career Group
Eight mid-career surgeons came up in two waves. The configuration was largely set by this point. The new work was around integration — anesthesia documentation needed to flow into the op-note draft, and the surgical-assistant notes needed to be linkable from the operative summary.
Weeks 6–9: The Junior Surgeons + ASC Workflow
The five junior surgeons came up last. They had the lowest resistance and the highest productivity ceiling. The final phase also closed the loop on the ASC-level workflow — operative reports were now flowing into the billing queue before the surgeon left the ASC for the day, enabling same-day claim submission for the first time.
Business Value
The CFO presented the results to the board in February 2026 — six months after go-live. The presentation was titled "The case for not hiring." It became the practice's most widely shared internal document.
What didn't happen
The practice did not hire two additional surgeons. The $3.2M in compensation, benefits, and support costs that the hire would have required was redirected into ASC capital equipment — including two new spinal-surgical robotics platforms that materially expanded the complexity ceiling of cases the practice could perform. Those platforms now drive incremental revenue on the existing surgeon base.
What changed about the strategic plan
The 2026 strategic plan was rewritten in early 2026 to reflect a different growth thesis. Instead of "add capacity through new surgeons," the new plan is "expand complexity through capital investment and operational efficiency." That thesis has held for two budget cycles.
What the senior surgeons say now
The surgeons are not publicly evangelical about the platform — they are surgeons, not marketers — but Dr. Reedman has been the keynote speaker at two orthopedic society annual meetings on the topic of practice operations. He doesn't pitch eCareScribe by name. He pitches the principle: the work that used to live in your evenings doesn't have to live there anymore. That has done more for Pinnacle's recruiting pipeline than any explicit advertising could.
The CFO's summary line
"We almost spent $3.2M to scale a problem instead of solving it. The platform didn't just save us the hiring cost — it saved us from compounding the cause of the hiring need."

